Anterior hip replacement surgery is a surgical approach that has been shown to provide many benefits over traditional hip replacement surgical approaches.
In this blog post, we will explore what exactly makes anterior hip replacement surgery different from traditional hip replacement surgery. We will also explain what the anatomy of the hip looks like, who is a good candidate for this approach, and what to expect from start to finish.
Anatomy of the Hip
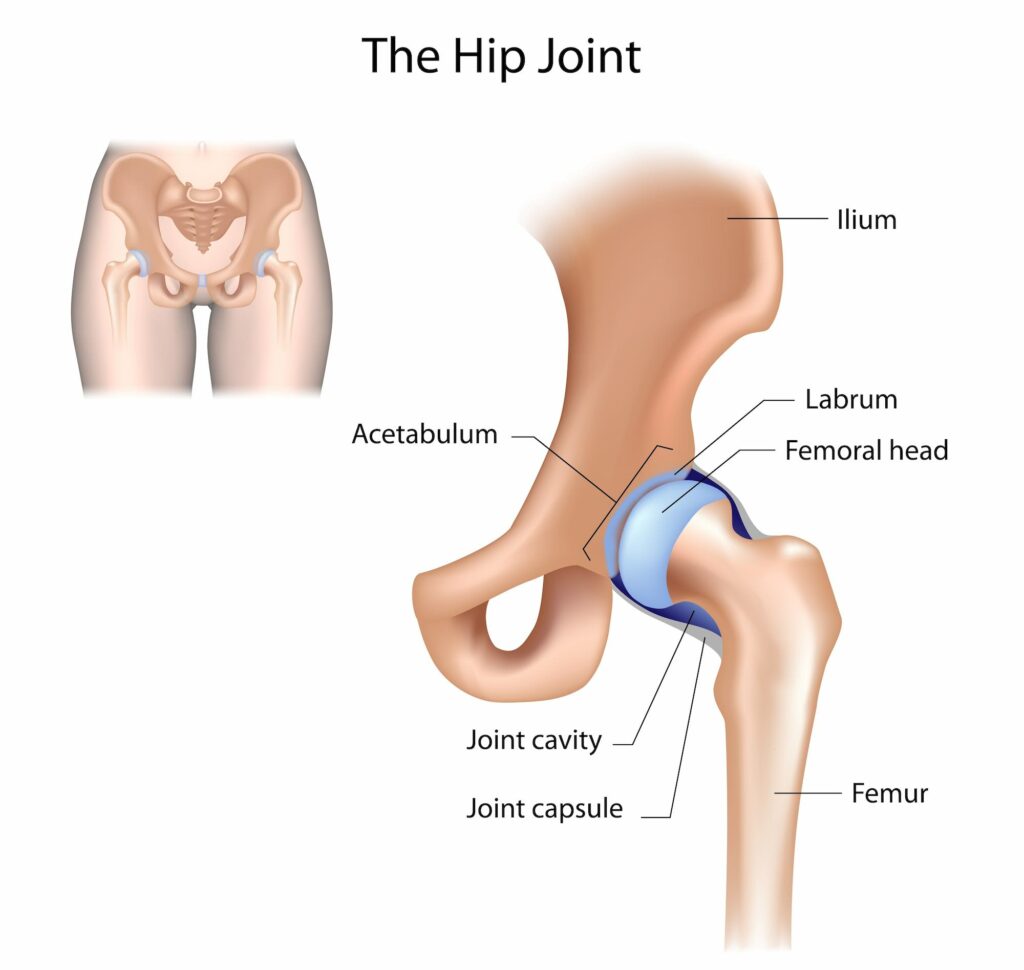
The hip joint is a ball and socket joint that is the point of articulation between the head of the femur and the acetabulum of the pelvis.
The “ball” which is known as the femoral head, sits in the acetabulum, or “the socket”. The femoral head is attached to the rest of the femur (thighbone) by a neck.
Two bones that make up the acetabulum are called the ilium and ischium. The ilium is the upper part of your hip bone that you can feel when you place your hand on your hip. The ischium is the lower, back part of your hip bone that you sit on. Both bones are connected by a pubic symphysis in the front.
The socket of the hip joint is lined with a smooth tissue called articular cartilage which covers the surface of the bones, allowing for a smooth gliding motion at the joint. These strong ligaments and muscles reinforce the hip joint and provide a great amount of stability and strength.
What Is Anterior Hip Replacement Surgery?
Anterior hip replacement surgery is a minimally invasive procedure to replace a damaged or arthritic hip joint. Unlike a traditional approach for a hip replacement where the incision is on the back or side of the hip, an anterior (front of the joint) hip replacement surgery is done with more specialized instruments and through a much smaller incision.
With the anterior approach, the patient is positioned in a way to facilitate various anatomical positions and enable the use of fluoroscopic imaging, ensuring the proper implant placement.
The surgeon makes the incision in front of the hip (about four inches long), starting at the front of the pelvic bone (iliac crest) and extending down toward the top of the thigh. This enables the surgeon to access the hip joint by spreading the muscles aside, rather than cutting them.
The femoral neck is then cut and the femoral head is removed from the acetabulum (the socket). The damaged cartilage surface of the socket is removed and replaced with a metal socket. Screws or cement are sometimes used to hold the socket in place. A liner made of either plastic, ceramic, or metal is inserted into the socket, creating a smooth gliding surface for the hip joint.
The damaged femoral head (ball) is removed and replaced with a metal stem that is placed into the prepared hollow center of the femur. The femoral stem may be either cemented or “press fit” into the bone.
Lastly, a metal or ceramic ball is the placed onto the upper part of the stem, replacing the damaged femoral head that was removed earlier in the procedure.
The surgeon will remove the instruments and depending on the individual, a drain may be inserted to help with possible swelling. The incision is then closed with sutures and covered with a sterile dressing.
Who Is a Candidate for Anterior Hip Replacement Surgery?
Dr. Jamieson has done anterior hip replacements on patients age ranging from mid 30’s to mid 90’s. Patients who suffer from hip pain that limits their daily activities, such as walking, climbing stairs, or getting in and out of a car, or stiffness that limits movement of the leg, may benefit from anterior hip replacement surgery. Inadequate pain relief from anti-inflammatory drugs, physical therapy, or walking supports may also qualify as a candidate. This type of surgery is typically recommended for, but not limited to, patients with osteoarthritis, rheumatoid arthritis, avascular necrosis, or hip fractures.
The Benefits of Anterior Hip Replacement Surgery Over Traditional Hip Replacement Surgery
Anterior hip replacement surgery has many potential benefits when compared to other hip replacement approaches. Traditional hip replacement approaches involves cutting through muscles and tendons to reach the hip joint, which can often lead to a more painful and longer recovery. With anterior hip replacement surgery, the muscles and tendons are not cut, but rather the surgeon uses the natural separation of the muscles to expose the joint. This allows the integrity of the hip muscles to stay in place, supporting the newly reconstructed hip joint and decreasing potential risks of dislocations.
The benefits of an anterior approach can result in less pain, quicker healing and quicker return to daily activities.
What to Expect During and After Anterior Hip Replacement Surgery
An anterior hip replacement surgery is typically rather quick, only taking about one to two hours to complete.
During the surgery, you will be given a spinal or general anesthesia to keep you asleep and pain-free. After the surgery is complete, you will be taken to a recovery room where you will be monitored until your blood pressure, heart rate, and breathing are stable. Provided there are no complications, and depending on your mobility, you will likely be sent home the same day. Some patients will be sent home the following day.
Some pain and discomfort is common after surgery and can be managed with pain medication. Patients who follow their surgeon’s post-operative guidelines may very likely return to their normal activities, including driving, within four to six weeks after surgery.

